Shoulder Internal Rotation Test
- Zielmuskel
- —
- Equipment
- Body weight
- Körperregion
- Stretching
- Typ
- Stretching
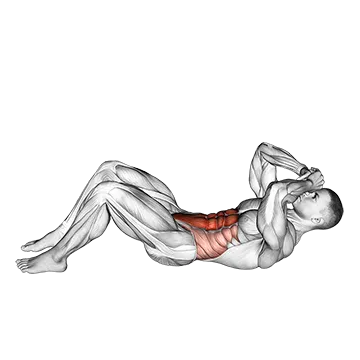
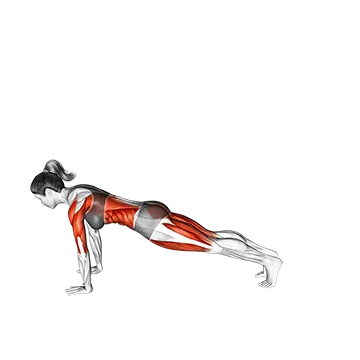
The Shoulder Internal Rotation Test is a bodyweight mobility assessment that measures how far the shoulder joint can rotate inward, identifying restrictions in the posterior capsule, infraspinatus, and teres minor. Performed supine with the arm at 90° abduction and elbow bent — or via the behind-the-back reach variation — it reveals asymmetries and range-of-motion deficits that often underlie shoulder pain and impingement. It is commonly used by athletes and clinicians to guide corrective stretching and rehabilitation programming.
Shoulder Internal Rotation Test: So führst du sie aus
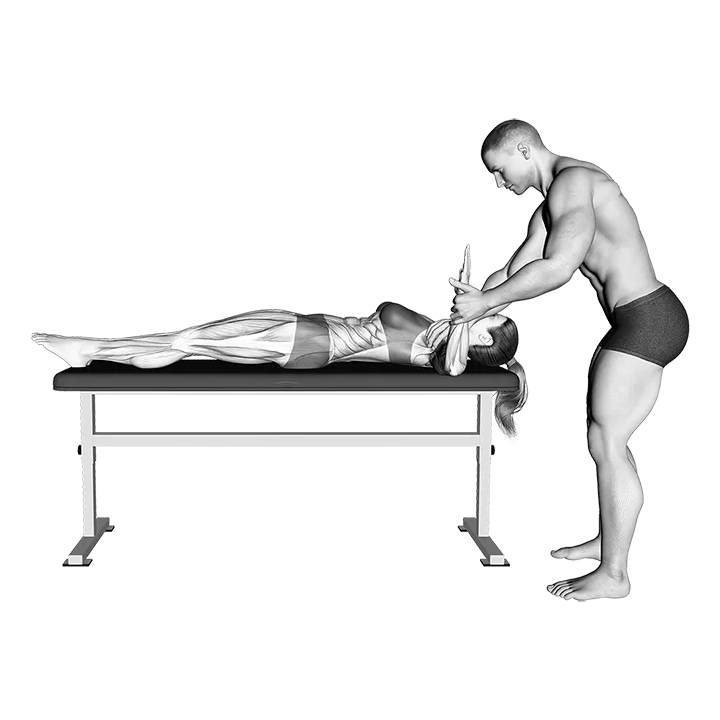
- 1Lie on your back on a firm, flat surface with your knees bent and feet flat on the floor.
- 2Raise your right arm out to the side until it is level with your shoulder — 90° of abduction — and bend your elbow to 90° so your forearm points straight up toward the ceiling.
- 3Allow your upper arm to rest fully on the floor; your elbow should stay in contact with the surface throughout the test.
- 4Keeping your elbow fixed and your upper arm pinned to the floor, slowly rotate your forearm forward and downward toward the floor — this is internal rotation.
- 5Stop when you feel resistance or when your elbow begins to lift off the surface, noting the angle your forearm makes with the floor.
- 6Hold the end-range position for 2–3 seconds to confirm this is your true limit, not muscular guarding.
- 7Return your forearm to the starting vertical position under control.
- 8Repeat the assessment on the left side and compare the range of motion between arms.
- 9Record any asymmetry greater than 10–15° or any reproduction of familiar pain as a positive finding warranting follow-up.
Technik-Tipps
- Keep your elbow firmly in contact with the floor throughout the movement — the moment it lifts, the test is no longer measuring pure glenohumeral internal rotation.
- Relax your hand and forearm completely during the test; gripping or tensing the hand engages forearm muscles that can artificially restrict or assist the motion.
- Breathe out slowly as you rotate downward to release muscular guarding and allow the shoulder to reach its true passive range.
- Always test both sides in the same session so you have a direct comparison — many shoulder dysfunctions present as side-to-side asymmetry rather than an absolute deficit.
- If you are using the behind-the-back variation, note the vertebral level your thumb reaches (e.g., T7) rather than estimating an angle for consistent tracking over time.
Häufige Fehler
- Letting the elbow lift off the floor: Once the elbow rises, the scapula compensates by tilting and the measurement reflects scapular mobility rather than glenohumeral rotation — anchor the elbow throughout the test.
- Rotating the trunk: Rolling the torso toward the rotating arm substitutes lumbar and thoracic movement for true shoulder internal rotation, artificially inflating the result and masking a real capsular restriction.
- Using excessive speed: Rapidly swinging the forearm down bypasses the posterior capsule's passive restraint; move slowly to accurately locate the true end range rather than bouncing through it.
- Skipping the contralateral comparison: Testing only one side provides no baseline — always compare both shoulders, as a deficit is often only meaningful when viewed relative to the non-dominant or asymptomatic side.
- Interpreting pain as normal end-feel: A sharp or pinching sensation at end range is not the same as the firm capsular resistance that signals normal end-of-range; pain during the test should be noted separately as it may indicate impingement or labral pathology.
Häufig gestellte Fragen
What is a normal range of motion for the shoulder internal rotation test?
Normal glenohumeral internal rotation with the arm at 90° abduction is typically 60–70° from vertical, meaning the forearm drops to within 20–30° of the floor. Athletes in overhead sports often show reduced internal rotation on their dominant side due to posterior capsule tightening — a side-to-side difference greater than 15–20° is generally considered a clinically meaningful deficit worth addressing.
What does it mean if I fail the shoulder internal rotation test?
A reduced result usually indicates tightness or thickening of the posterior glenohumeral capsule, along with shortened infraspinatus and teres minor muscles. This pattern — sometimes called glenohumeral internal rotation deficit (GIRD) — is common in overhead athletes and can contribute to impingement, SLAP tears, and rotator cuff irritation. A positive test warrants targeted posterior capsule stretching such as the sleeper stretch, and potentially a physiotherapy assessment.
How is the shoulder internal rotation test different from the sleeper stretch?
The shoulder internal rotation test is a passive assessment used to quantify your current range of motion; no stretch is applied beyond your end range. The sleeper stretch is a therapeutic stretch that uses gentle overpressure at end range to improve posterior capsule mobility over time. The test tells you what your baseline is; the sleeper stretch is the corrective intervention you use to improve it.
Can I perform the shoulder internal rotation test at home without equipment?
Yes. The supine version requires only a firm, flat surface such as a yoga mat or hardwood floor — no equipment whatsoever. Lie down, position your arm at 90° abduction and 90° elbow flexion, and slowly rotate your forearm toward the floor. A partner can help observe the angle and whether your elbow stays grounded, but the test is entirely self-administrable.
How often should I retest shoulder internal rotation to track progress?
Retest every 4–6 weeks if you are actively working on posterior capsule mobility. Testing too frequently (e.g., weekly) rarely shows meaningful change and can become discouraging. Record results each time — noting forearm angle or distance from the floor — so you have an objective comparison rather than relying on feel alone.